These medications are considered safe in pregnancy with the included guidance:
- Cyclosporin/Tacrolimus: monitor blood pressure
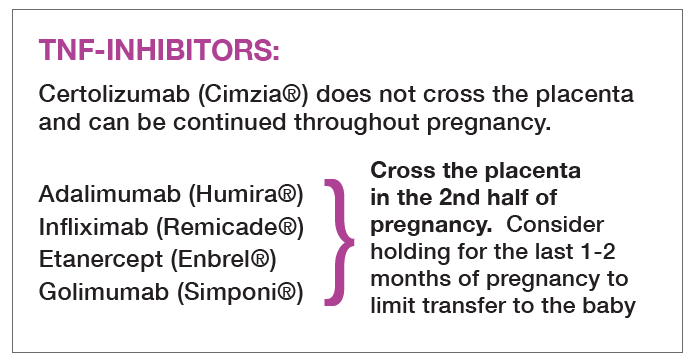
- Infliximab, Etanercept, Golimumab, Adalimumab: discontinue several half-lives prior to delivery
- Rituximab: only in very active rheumatic disease
Following the publication of the ACR Reproductive Health Guidelines in 2020, the FDA issued a Black Box Warning against the use of NSAIDs in pregnancy.
- NSAIDs (Meloxicam, Ibuprofen, Naproxen, etc.): consult with obstetrician before use in pregnancy